


“… in the face of such patients, it is necessary to be vigilant to the new type of coronavirus infection that can affect the central nervous system…”

Beijing Ditan Hospital affiliated to the Capital Medical University said on March 4 that the first patient with novel coronavirus pneumonia complicated with encephalitis was discharged from the hospital on February 25.
Liu Jingyuan, director of the ICU at the Hospital, presided over the treatment of the patient. He reminded that patients with conscious disturbances must consider the possibility that the virus may attack the central nervous system.
At present, patients with new type of coronavirus pneumonia can be combined with multiple organ damages such as severe respiratory distress syndrome (ARDS), myocardial damage, abnormal coagulation function, kidney damage, liver damage, etc. However, no central nervous system involvement has been reported. The case report is the first in the world.
Previous studies on SARS (Severe Acute Respiratory Syndrome) and MERS (Middle East Respiratory Syndrome) have also shown that the coronaviruses that cause these two diseases also cause cases of central nervous system damage.
According to the introduction of Beijing Ditan Hospital, two suspected cases of new-type coronavirus pneumonia have been treated since January 12 this year (confirmed on January 20). As of 7:00 on March 4, the hospital has accumulatively received 150 patients with new-type coronavirus pneumonia, of which the above patient is the only patient with new type of coronavirus pneumonia and encephalitis.
The 56-year-old patient was admitted to the hospital on January 24 with new coronavirus pneumonia, critical illness, and respiratory failure. After admission, he was given a combination of interferon nebulization, antiviral treatment, prevention of bacterial infection, and TCM syndrome differentiation. No improvement, high fever, fatigue, and dyspnea gradually increased.
On January 27 (10th day of onset), a chest CT showed that the range of ground-glass density in both lungs was enlarged, and some of them were consolidating. Short-term nasal high-flow oxygen inhalation, no relief in breathing distress, irritability, breathing 50 breaths per minute, partial oxygen pressure of 85%, intubation in the ICU, mechanical ventilation in accordance with the principle of ARDS breathing ventilation.
After 96 hours of treatment (day 14 of the onset), the patient developed frequent twitching of the maxillofacial and mouth angles with persistent hiccups.
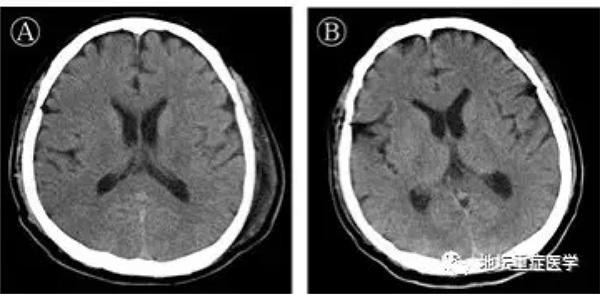
On examination, the doctor found positive neck resistance, bilateral pupils and other large contours, sluggish light reflection, increased limb muscle tension, bilateral knee reflexes, bilateral Pap sign and ankle clonus, and no intracranial CT scan. Abnormal, the cerebrospinal fluid pressure was greater than 330mmH2O, the appearance of the cerebrospinal fluid was colorless and clear, and the biochemical test was normal.
Beijing Ditan Hospital’s Department of Critical Medicine, Laboratory Medicine, and the China Centers for Disease Control and Prevention’s Infectious Diseases Joint Working Group performed metagenome second-generation sequencing of the collected cerebrospinal fluid specimens and identified possible infectious pathogens. Other pathogens were excluded and a new coronavirus was obtained. Genomic sequence.
Gene sequencing confirmed the existence of a new coronavirus in the cerebrospinal fluid and clinical diagnosis of viral encephalitis.
Subsequently, the medical staff treated the patients with viral encephalitis after 14 days of mechanical ventilation and mannitol to control intracranial pressure, midazolam to control convulsions, gamma globulin, and methylprednisolone anti-inflammatory treatment, and observed the patient’s lung disease imaging gradually. Improved, neurological symptoms disappeared.
On February 10 (day 24 of the onset of illness), the trachea was intubated and the nasal cannula was given oxygen after fully assessing the patient’s respiratory and neural function. On February 18 (the 32nd day after the onset of illness), he was transferred out of the intensive care unit and continued to receive treatment in the new coronavirus ward.
Liu Jingyuan reminded that in clinical observation, there were many cases of cervical resistance, positive pathological signs, sudden disturbance of consciousness and even coma.
He said that in the face of such patients, it is necessary to be vigilant to the new type of coronavirus infection that can affect the central nervous system, timely conduct relevant examinations such as cerebrospinal fluid, and improve the work on SARS-CoV-2 nucleic acid and gene sequencing of cerebrospinal fluid in order to better understand COVID-19. Explore and actively deal with related neurological complications, thereby further reducing the mortality of critically ill patients.